






Authors: Nicholas S. Imperato DO, MPH (@nickimperato14, Emergency Medicine Resident, Rutgers New Jersey Medical School), Cynthia Santos MD (Associate Professor, Emergency Medicine, Medical Toxicology, Addiction Medicine, Rutgers New Jersey Medical School) // Reviewed by: Ann-Jeannette Geib, MD (Associate Professor, Emergency Medicine, Medical Toxicology, Wake Forest University School of Medicine, Carolinas Medical Center); Brit Long, MD (@long_brit)

Case:
A 25-year-old male presents to the Emergency Department (ED) after falling from a 10-foot ladder with an obvious deformity to the left arm. After the initial workup, which included imaging, he was found to have a distal radius fracture. Throughout the encounter, the patient was visibly uncomfortable despite various oral analgesics, and he continued to rate the pain as a 10 out of 10. Given concerns about potential adverse effects from higher doses of opioid analgesia and the need for rapid pain control, the ED team considered using inhaled nitrous oxide (N₂O) for the management of his acute pain.
Questions:
- How does nitrous oxide provide analgesic effects?
- What are the potential adverse effects or contraindications to its use?
- What patient populations or clinical scenarios may benefit most from nitrous oxide for acute pain management in the ED?
Background:
Nitrous oxide (N₂O), more commonly known as “laughing gas,” has been used for years as an analgesic in both adults and children due to its rapid onset, low solubility, and relative ease of administration. It has analgesic, anxiolytic, and amnestic properties, which may reduce the need for additional analgesics. However, its mild anesthetic properties make it insufficient for deep anesthesia on its own. Due to its low potency and rapid onset and recovery, it is commonly used alongside stronger anesthetic agents. Often combined with oxygen (O2), it serves as a mild sedative with analgesic effects and is frequently utilized in dentistry and minor medical procedures. In the ED, it is particularly useful for short, painful procedures such as fracture reductions, laceration repairs, and burn dressings. Of the inhalational anesthetics, nitrous oxide is the least potent and has minimal hemodynamic effects.1
Nitrous oxide modulates pain through multiple pathways and is believed to antagonize NMDA (N-methyl-D-aspartate) receptors in the central nervous system while increasing endogenous opioid release, producing significant analgesic effects with minimal sedation. Nitrous oxide also activates GABA receptors, allowing for its anxiolytic properties. It is rapidly absorbed through alveoli when inhaled and has an onset of action between 2 and 5 minutes.1
Epidemiology
- Global Use: In dental offices across the world, nitrous oxide is regularly utilized for analgesia and anxiolysis, but over the past few decades, its use in EDs, and specifically pediatric EDs, has grown.2,3
- Current Trends: More frequent use in EDs has led to the development and introduction of portable N₂O delivery systems, which allow for straightforward and more rapid administration for acute injuries or painful procedures.
Clinical Uses
Patients with acute injuries may benefit from N₂O administration for pain relief prior to or during procedures.4 N₂O is often utilized for:
- Fracture Reduction
- Laceration Repair or Wound Care
- Burn Management: Dressing changes or debridement
- Other Painful Procedures: Placement of nasogastric tubes or intravenous lines in anxious patients
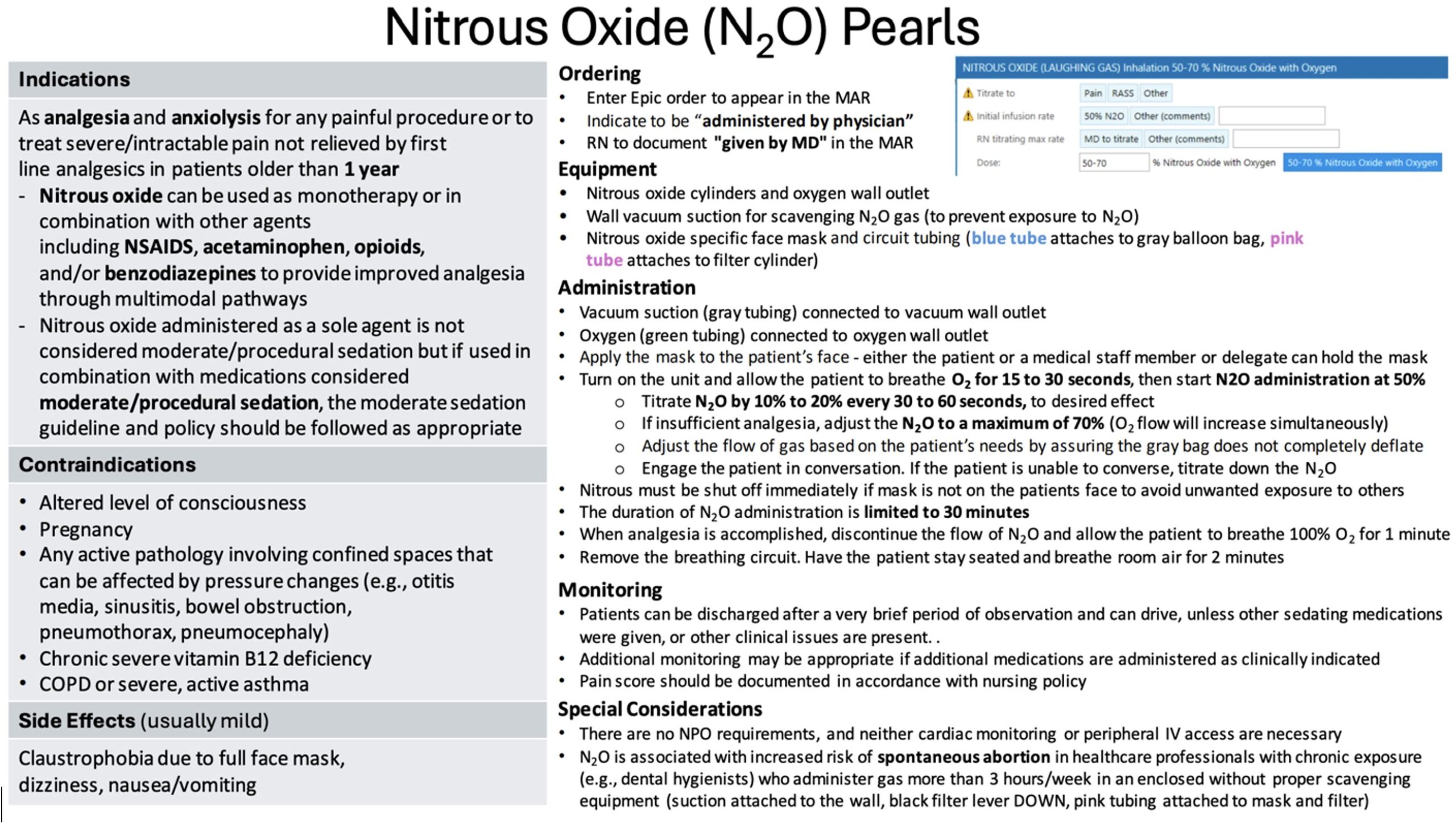
Indications
- Any painful procedure in a patient over the age of 1
Contraindications
- Altered mental status
- Active pathology that could potentially be affected by pressure changes (otitis media, sinusitis, bowel obstruction, pneumothorax, pneumocephaly)
- Chronic severe vitamin B12 deficiency
- COPD
- Severe asthma exacerbation
- First or second trimester of pregnancy*
*Nitrous oxide has been utilized for pain relief during labor in pregnant women. However, chronic exposure to N₂O without adequate scavenging equipment may pose reproductive risks, including an increased risk of miscarriage. Proper ventilation and scavenging systems are essential to minimize occupational exposure and safeguard both healthcare workers and patients.5
Management/Set-Up
- Preparation
- Ensure that you have access to proper equipment (e.g., a N2O/O2 delivery system with scavenging) and appropriate monitoring (e.g., pulse oximetry, blood pressure, and heart rate)
- N₂O is self-administered; therefore, check that the patient can hold the nitrous oxide mask
- Educate the patient prior to use regarding what to expect (e.g., tingling, lightheadedness)
- Administration
- Inhaled N₂O/O₂ Mixture: Often, a 50% N₂O and 50% O₂ blend is used, providing rapid onset (1-3 minutes) and quick offset once inhalation ceases. Nitrous oxide-oxygen delivery systems are typically limited to a maximum of 70% N₂O and 30% O₂. Side effects of N₂O are reduced if administered for less than 30 minutes
- Sedation Depth Monitoring: Minimal sedation with rapid recovery
- Adjunctive Analgesia
- Additional analgesics (e.g., NSAIDs, acetaminophen, opioids) may be used depending on the severity of pain and clinical judgment
- Post-Procedure Care
- Observe for adverse effects such as nausea, vomiting, or dizziness
- Have the patient sit and breathe room air for 2 minutes
- Further observation or additional monitoring is not necessary
ACEP Acute Pain Toolkit: Acute Pain (MAP) | ACEP
Hospital Guideline (University Hospital (Newark, NJ) Emergency Department guidelines for the use of nitrous oxide)
Case Follow-up:
The patient tolerated the N₂O well and reported that pain was significantly reduced while using it during the fracture reduction. The patient remained hemodynamically stable throughout the reduction and only reported mild lightheadedness that resolved spontaneously within minutes after the N₂O was removed. He was then discharged with an outpatient pain control regimen and orthopedic surgery follow-up.
Clinical Pearls:
- Rapid Onset and Offset: Nitrous oxide provides quick analgesia and wears off rapidly once administration stops
- Titration and Self-Administration: Patients can titrate and use as needed throughout the procedure
- Potential Contraindications: Avoid use of nitrous oxide in cases of otitis media, sinusitis, pneumothorax, or severe COPD exacerbations. Although nitrous oxide has been used to treat labor pain, there is limited data on its effects on fetal development, so it should be avoided in 1st and 2nd trimester pregnancy. Limited data are showing an increased risk of spontaneous abortion in healthcare workers regularly exposed to nitrous oxide without proper scavenging equipment
- Minimal Sedation Profile: Patients are able to maintain airway reflexes and protective mechanisms, making it safer when compared to deeper sedation options
- Adjunct to Multimodal Analgesia: Nitrous oxide can reduce the required dose of opioids, lowering the risk of opioid-related side effects
References
- Knuf, K., & Maani, C. V. (2023). Nitrous Oxide. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK532922/
- Roberts, G. J. (1990). Inhalation sedation (relative analgesia) with oxygen/nitrous oxide gas mixtures: 1. Principles. Dental Update, 17(4), 139–142, 145–146.
- Veger, M. L., van Iterson, J., Bakx, R., & Ridderikhof, M. L. (2024). The Role of Nitrous Oxide in Minor Pediatric Procedures in the Emergency Department: A Systematic Review. Journal of Pediatric Surgery, 59(6), 1154–1162. https://doi.org/10.1016/j.jpedsurg.2023.12.026
- Huang, C., & Johnson, N. (2016). Nitrous Oxide, From the Operating Room to the Emergency Department. Current Emergency and Hospital Medicine Reports, 4, 11. https://doi.org/10.1007/s40138-016-0092-3
- Vallejo MC, Zakowski MI. Pro-Con Debate: Nitrous Oxide for Labor Analgesia. Biomed Res Int. 2019 Aug 20;2019:4618798. doi: 10.1155/2019/4618798. PMID: 31531352; PMCID: PMC6720045.



